


















The main criterionarterial hypertension (or arterial hypertension)as a whole group of diseases - stable, that is, detected through repeated measurements on different days, an increase in blood pressure (BP).The question of what kind of blood pressure is considered elevated is not as simple as it may seem.The fact is that among practically healthy people the range of blood pressure values is quite wide.The results of long-term observation of people with different levels of blood pressure showed that already starting from the level of 115/75 mm Hg.Art., each additional increase in blood pressure by 10 mm Hg.Art.is associated with an increased risk of developing cardiovascular diseases (mainly coronary heart disease and stroke).However, the benefits of modern methods of treating arterial hypertension have been proven mainly only for those patients whose blood pressure exceeded 140/90 mmHg.Art.For this reason, it was agreed that this threshold value should be considered as a criterion for the identification of arterial hypertension.
Increased blood pressure can be associated with dozens of different chronic diseases, and hypertension is only one of them, but the most common: approximately 9 cases out of 10. The diagnosis of hypertension is made in cases where there is a steady increase in blood pressure, but no other diseases that lead to increased blood pressure are detected.
Hypertension is a disease for which a steady increase in blood pressure is its main manifestation.Risk factors that increase the likelihood of its development have been determined through observations of large groups of people.In addition to the genetic predisposition that some people have, these risk factors include:
- obesity;
- passivity;
- excessive consumption of table salt, alcohol;
- chronic stress;
- smoking.
In general, all those features that accompany the modern urban lifestyle in industrialized countries.This is why hypertension is considered a lifestyle disease and targeted changes for the better should always be considered as part of a case-by-case hypertension treatment program.
What other diseases are associated with increased blood pressure?These are many kidney diseases (pyelonephritis, glomerulonephritis, polycystic disease, diabetic nephropathy, stenosis (narrowing) of the renal arteries, etc.), a number of endocrine diseases (kidney tumors, hyperthyroidism, Cushing's disease and syndrome), obstructive sleep apnea syndrome and some other rare diseases., Regular use of medications such as glucocorticosteroids, non-steroidal anti-inflammatory drugs and oral contraceptives can alsolead to a continuous increase in blood pressure.The diseases and conditions listed above lead to the development of so-called secondary or symptomatic arterial hypertension.The doctor makes a diagnosis of hypertension if during a conversation with the patient, ascertaining the history of the disease, the examination, as well as based on the results of several research methods, mainly simple laboratory and instrumental, the diagnosis of any of the secondary arterial hypertension seems impossible.
If you notice similar symptoms, consult your doctor.Do not self-medicate - it is dangerous for your health!
Symptoms of arterial hypertension
High blood pressure itself does not manifest itself in any subjective sensations for many people.If high blood pressure is accompanied by symptoms, this may include a feeling of heaviness in the head, headache, flashing eyes, nausea, dizziness, unsteadiness while walking, as well as a number of other symptoms that are quite non-specific to high blood pressure.The symptoms listed above appear much more clearly during a hypertensive crisis - a sudden significant increase in blood pressure, which leads to a clear deterioration of the condition and well-being.
It would be possible to continue to list possible symptoms of hypertension, separated by commas, but there is no particular benefit in doing so.Why?Firstly, all these symptoms are non-specific for hypertension (that is, they can occur individually or in various combinations in other diseases), and secondly, to prove the presence of arterial hypertension, the very fact of a steady increase in blood pressure is important.And this is revealed not by evaluating subjective symptoms, but only by measuring blood pressure, moreover, repeatedly.This means, first, that "in one sitting" blood pressure should be measured two or three times (with a short break between measurements) and the arithmetic mean of two or three measured values should be taken as the true blood pressure.Second, the stability of the increase in blood pressure (criteria for diagnosing hypertension as a chronic disease) should be confirmed by measurements on different days, preferably with an interval of at least one week.
If a hypertensive crisis develops, there will definitely be symptoms, otherwise it is not a hypertensive crisis, but simply an asymptomatic increase in blood pressure.And these symptoms can be either those listed above or other, more serious ones - they are discussed in the "Complications" section.
Symptomatic (secondary) arterial hypertension develops as part of other diseases, and therefore their manifestations, in addition to the actual symptoms of high blood pressure (if any), depend on the underlying disease.For example, with hyperaldosteronism, this can be muscle weakness, cramps and even temporary paralysis (lasting hours or days) in the muscles of the legs, arms and neck.With obstructive sleep apnea syndrome - snoring, sleep apnea, daytime sleepiness.
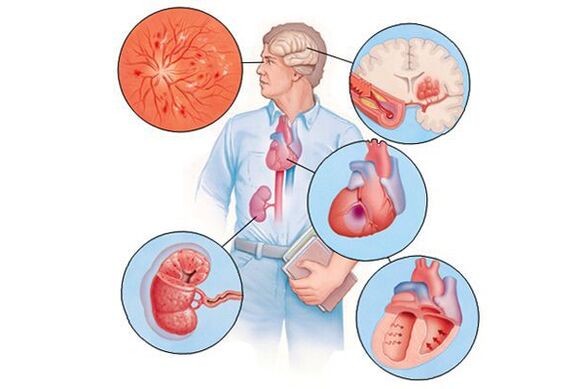
If hypertension over time - usually many years - leads to damage to various organs (in this context they are called "target organs"), then this can appear as a decrease in memory and intelligence, stroke or transient cerebrovascular accident, increase in the thickness of the heart walls, accelerated development of atherosclerotic plaques in the heart vessels and other organic vessels.reduction of the rate of blood filtration in the kidneys, etc.Therefore, the clinical manifestations will be caused by these complications and not by the increase in blood pressure as such.
Pathogenesis of arterial hypertension
In hypertension, the disorder of vascular tone and the increase in blood pressure are the main content of this disease, so to speak, its "quintessence".Factors such as genetic predisposition, obesity, inactivity, excessive consumption of table salt, alcohol, chronic stress, smoking and a number of others, mainly related to lifestyle characteristics, lead over time to the disruption of the functioning of the endothelium - the inner layer of arterial vessels with a thick cell layer, which is actively involved in the regulation of blood tone and blood vessels.The tone of microvascular vessels, and thus the volume of local blood flow in organs and tissues, is regulated autonomously by the endothelium and not directly by the central nervous system.This is a system of local regulation of blood pressure.However, there are other levels of blood pressure regulation - the central nervous system, the endocrine system and the kidneys (which also understand their regulatory role mainly due to the ability to participate in hormonal regulation at the level of the whole organism).Violations in these complex regulatory mechanisms lead, in general, to a decrease in the ability of the entire system to adapt well to the constantly changing needs of organs and tissues for blood supply.
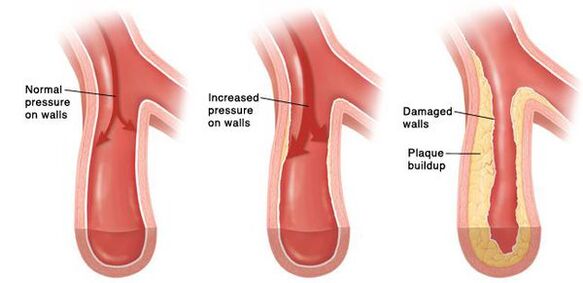
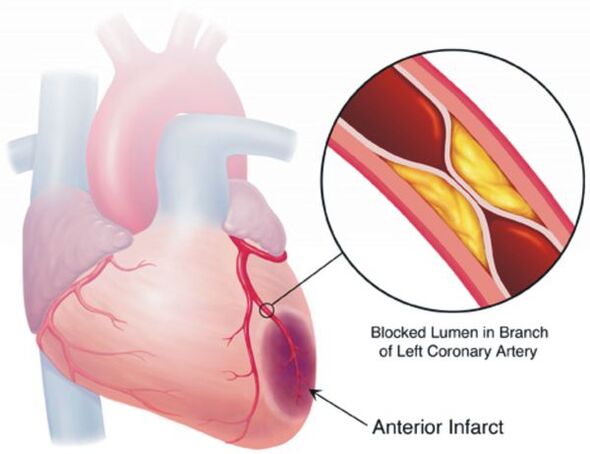
Over time, a constant spasm of the small arteries develops, and then their walls change so much that they are no longer able to return to their original state.In larger vessels, due to the continuous increase in blood pressure, atherosclerosis develops at an accelerated rate.The walls of the heart become thicker, hypertrophy of the myocardium develops, and then the expansion of the cavities of the left atrium and the left ventricle.The increased pressure damages the glomeruli, their number decreases and therefore the kidney's ability to filter blood decreases.In the brain, due to changes in the blood vessels that supply it, negative changes also occur - small foci of hemorrhages appear, as well as small areas of necrosis (death) of brain cells.When an atherosclerotic plaque ruptures in a sufficiently large vessel, thrombosis occurs, the lumen of the vessel is blocked, and this leads to a stroke.
Classification and stages of development of arterial hypertension
Hypertension, depending on the magnitude of high blood pressure, is divided into three degrees.Also, taking into account the increase in the risk of cardiovascular diseases on a "year-decade" scale, already starting from a blood pressure level above 115/75 mm Hg.Art., there are several other scales of blood pressure levels.
If the values of systolic and diastolic blood pressure fall into different categories, then the degree of arterial hypertension is estimated by the higher value of the two values, and it does not matter - systolic or diastolic.The rate of increase in blood pressure during the diagnosis of hypertension is determined by repeated measurements on different days.
In some countries, the stages of hypertension continue to be distinguished, while the European guidelines for the diagnosis and treatment of arterial hypertension do not mention any stage.The identification of stages aims to reflect the stage of the course of hypertension from its onset to the appearance of complications.
There are three stages:
- Phase Imeans that there are still no visible damages in those organs that are most often affected by this disease: there is no enlargement (hypertrophy) of the left ventricle of the heart, there is no significant decrease in the filtration rate in the kidneys, which is determined by taking into account the level of creatinine in the blood, albumin protein is not detected in the urine, thickening of the skin walls or thickening of the plaques in them is not detected, etc.Such damage to internal organs is usually asymptomatic.
- If there is at least one of the listed signs, make the diagnosisPhase IIhypertension.
- Finally, approxPhase IIIHypertension is called when there is at least one cardiovascular disease with clinical manifestations associated with atherosclerosis (myocardial infarction, stroke, angina pectoris, atherosclerotic lesions of the arteries of the lower extremities), or, for example, serious kidney damage, manifested by a marked decrease in protein filtration and/or significant protein loss.
These stages do not always naturally replace each other: for example, a person suffered a myocardial infarction and after a few years an increase in blood pressure occurred - it turns out that such a patient immediately has stage III hypertension.The purpose of staging is primarily to rank patients according to their risk for cardiovascular complications.Treatment measures also depend on this: the higher the risk, the more intensive the treatment.When a diagnosis is formulated, the risk is assessed on four levels.At the same time, the 4th grade corresponds to the greatest risk.
Complications of arterial hypertension
The goal of treating hypertension is not to "lower" high blood pressure, but to maximally reduce the risk of cardiovascular and other complications in the long term, since this risk—again, when evaluated on a "year-decade" scale—increases for every additional 10 mm Hg.Art.already from the blood pressure level of 115/75 mm Hg.Art.This refers to complications such as stroke, coronary heart disease, vascular dementia (dementia), chronic renal and chronic heart failure, atherosclerotic vascular lesions of the lower extremities.
Most patients with hypertension are not worried about anything at the moment, so they do not have much motivation to treat themselves, regularly taking a certain minimum of medication and changing their lifestyle in a healthier way.However, in the treatment of hypertension there are no one-time measures that will allow you to forget about this disease forever without doing anything more to treat it.
Diagnosis of arterial hypertension
With the diagnosis of arterial hypertension as such, everything is usually quite simple: it only requires repeatedly recorded blood pressure at the level of 140/90 mm Hg.Art.and above.But hypertension and arterial hypertension are not the same thing: as already mentioned, an increase in blood pressure can appear in a number of diseases, and hypertension is only one of them, although the most common.When making a diagnosis, the doctor, on the one hand, must make sure that the increase in blood pressure is stable, and on the other hand, assess the likelihood that the increase in blood pressure is a manifestation of symptomatic (secondary) arterial hypertension.
To do this, in the first stage of diagnostic research, the doctor finds out at what age the blood pressure began to rise, if there are symptoms such as, for example, snoring with pausesin breathing during sleep, attacks of muscle weakness, unusual impurities in the urine, attacks of sudden palpitations with sweating and headache, etc.It is reasonable to clarify what medications and dietary supplements the patient is taking, because in some cases they can lead to an increase in blood pressure or worsening of an already existing blood pressure.Some routine diagnostic tests (performed in almost all patients with high blood pressure), together with the information obtained during a conversation with a doctor, help to assess the likelihood of some forms of secondary hypertension: a complete analysis of urine, determination of the concentration of creatinine and glucose in the blood, and sometimes potassium and other electrolytes.In general, taking into account the low prevalence of secondary forms of arterial hypertension (about 10% of all its cases), further research of these diseases as a possible cause of high blood pressure should have good reasons.Therefore, if at the first stage of diagnostic research no significant data are found in favor of the secondary nature of arterial hypertension, then in the future it is considered that the blood pressure increases due to hypertension.This judgment can sometimes be revised later when new information about the patient becomes available.
In addition to searching for data on the possible secondary nature of increased blood pressure, the doctor determines the presence of risk factors for cardiovascular diseases (this is necessary to assess the prognosis and a more targeted search for damage to internal organs), as well as, possibly, pre-existing diseases of the cardiovascular system or their asymptomatic damage - this affects the assessment of the prognosis and the choice of hypertension.measures.For this, in addition to talking with the patient and examining him, a number of diagnostic studies are performed (for example, electrocardiography, echocardiography, ultrasound examination of the vessels of the neck and, if necessary, some other studies, the nature of which is determined by the medical data already obtained for the patient).

Daily monitoring of blood pressure using special compact devices allows you to assess changes in blood pressure during the patient's usual lifestyle.This study is not necessary in all cases - mainly, if the blood pressure measured at the doctor's appointment differs significantly from that measured at home, if it is necessary to evaluate the blood pressure at night, if hypotensive episodes are suspected and sometimes to evaluate the effectiveness of the treatment.
Thus, some diagnostic methods during the examination of a patient with high blood pressure are used in all cases;the use of other methods is more selective, depending on the data already obtained for the patient, to check the assumptions that the doctor made during the preliminary examination.
Treatment of arterial hypertension
In relation to non-drug measures aimed at treating hypertension, the most convincing evidence has been accumulated on the positive role of reducing salt intake, reducing and maintaining body weight at this level, regular physical exercise (exertion), no more than moderate alcohol consumption, and increasing the content of vegetables and fruits in the diet.Only all these measures are effective as part of long-term changes in the unhealthy lifestyle that led to the development of hypertension.For example, a decrease in body weight of 5 kg led to a decrease in blood pressure by an average of 4.4/3.6 mmHg.Art.- It seems little, but in combination with the other measures listed above to improve the lifestyle, the effect can be quite significant.
Lifestyle improvement is warranted for almost all patients with hypertension, but drug treatment is indicated, although not always, in most cases.If patients with an increase in blood pressure of 2 and 3 degrees, as well as with hypertension of any degree with a high calculated cardiovascular risk, drug treatment is mandatory (its long-term benefit has been demonstratedin many clinical studies), then in grade 1 hypertension with calculated low and moderate cardiovascular risk, the benefit of such treatment has not been convincingly established in large clinical trials.In such situations, the potential benefit of drug therapy is evaluated individually, taking into account the patient's preferences.If, despite the improvement of the lifestyle, the increase in blood pressure in such patients continues for several months during repeated visits to the doctor, it is necessary to reassess the need for the use of medication.Moreover, the magnitude of the calculated risk often depends on the completeness of the patient's examination and may turn out to be significantly higher than originally thought.In almost all cases of hypertension treatment, they try to achieve stabilization of blood pressure below 140/90 mm Hg.Art.This does not mean that in 100% of the measurements it will be below these values, but the less often the blood pressure, when measured under standard conditions (described in the "Diagnostics" section), crosses this threshold, the better.Thanks to this treatment, the risk of cardiovascular complications is significantly reduced and hypertensive crises, if they occur, are much less common than without treatment.Thanks to modern medications, those negative processes that in hypertension inevitably and latently destroy the internal organs over time (mainly the heart, brain and kidneys), these processes are slowed down or suspended, and in some cases can even be reversed.
Of the medications for the treatment of hypertension, the main ones are 5 classes of drugs:
- diuretics (diuretics);
- calcium antagonists;
- angiotensin-converting enzyme inhibitors (names ending in -adj);
- angiotensin II receptor antagonists (names ending in -sartan);
- beta blockers.
Recently, the role of the first four classes of drugs in the treatment of hypertension has been particularly emphasized.Beta-blockers are also used, but mainly when their use is required by co-morbidities – in these cases, beta-blockers have a dual purpose.
Nowadays, combinations of drugs are preferred, since treatment with any one of them rarely leads to achieving the desired level of blood pressure.There are also fixed combinations of drugs that make the treatment more convenient, since the patient only takes one tablet instead of two or even three.The choice of the necessary classes of drugs for a given patient, as well as the doses and frequency of their administration, is made by the doctor, taking into account such data about the patient as the level of blood pressure, concomitant diseases, etc.
Thanks to the multifaceted positive effects of modern drugs, the treatment of hypertension includes not only the reduction of blood pressure as such, but also the protection of internal organs from the negative effects of those processes that accompany high blood pressure.In addition, since the main goal of treatment is to minimize the risk of its complications and increase life expectancy, it may be necessary to correct the level of cholesterol in the blood, take medications that reduce the risk of blood clotting (leading to myocardial infarction or stroke), etc.Quitting smoking, no matter how trivial its risk may sound.heart attack associated with hypertension and slow down the growth of atherosclerotic plaques in the blood vessels.Thus, the treatment of hypertension involves treating the disease in many ways, and achieving normal blood pressure is only one of them.
The prediction.Preventing
The general prognosis is determined not only and not so much by the fact of high blood pressure, but by the number of risk factors for cardiovascular diseases, their degree of severity and the duration of the negative impact.
These risk factors are:
- smoking;
- increased blood cholesterol levels;
- high blood pressure;
- obesity;
- sedentary lifestyle;
- age (with each decade lived after 40 years, the risk increases);
- male gender and others.
In this case, not only the intensity of exposure to risk factors matters (for example, smoking 20 cigarettes a day is definitely worse than 5 cigarettes, although both are associated with a worse prognosis), but also the duration of their exposure.For people who do not yet have obvious cardiovascular disease other than hypertension, prognosis can be estimated using special electronic calculators, one of which takes into account gender, age, blood cholesterol level, blood pressure and smoking.The SCORE electronic calculator is suitable for estimating the risk of death from cardiovascular disease in the next 10 years from the date of the risk assessment.At the same time, the risk taken in most cases, which is low in absolute numbers, can create a misleading impression, because the Calculator allows you to calculate the risk of cardiovascular death.The risk of non-fatal complications (myocardial infarction, strokes, angina pectoris, etc.) is many times higher.The presence of diabetes mellitus increases the risk compared to that calculated using a calculator: for men 3 times, and for women - even 5 times.
Regarding the prevention of hypertension, we can say that since the risk factors for its development are known (inactivity, excess weight, chronic stress, regular lack of sleep, alcohol abuse, increased consumption of salt in food and others), then all lifestyle changes that reduce the impact of these factors also reduce the risk of developing hypertension.However, it is hardly possible to completely reduce this risk to zero - there are factors that do not depend on us at all or depend a little on us: genetic characteristics, gender, age, social environment and some others.The problem is that people start thinking about preventing hypertension mainly when they are already sick, and the blood pressure has already increased to one degree or another.And this is not so much a matter of prevention as of treatment.